修正手術個案 · 胃食道逆流
Revisional Surgery · Refractory GERD
「我終於能好好
躺平睡一覺了!」
"I can finally sleep
flat on my back again."
五年前接受縮胃曠腸手術,此後反覆胃食道逆流、固體食物難以下嚥,夜夜只能半坐著入睡。輾轉來到高雄長庚,一次腹腔鏡修正手術,五年的噩夢終於結束。
Five years after a sleeve gastrectomy with jejunal bypass, she was still battling relentless acid reflux, could barely eat solid food, and had spent years sleeping semi-upright. One revisional operation at Kaohsiung Chang Gung brought five years of suffering to an end.
50 歲女性
Female, 50s
修正手術
Revisional Surgery
食道裂孔疝氣復發
Recurrent Hiatal Hernia
Transit Bipartition
📅 五年的歷程
Five-Year Journey
第 0 年 ── 初次手術
Year 0 — Initial Surgery
縮胃曠腸手術(Sleeve Gastrectomy + Proximal Jejunal Bypass)
Sleeve Gastrectomy + Proximal Jejunal Bypass
於他院接受減重手術,術式為縮胃合併近端空腸曠置,初期減重效果可接受。
Bariatric surgery performed at another institution. Sleeve gastrectomy combined with proximal jejunal bypass; initial weight loss was satisfactory.
第 2 年 ── 症狀惡化
Year 2 — Deterioration
嚴重胃食道逆流、接受食道裂孔疝氣修補
Severe GERD Develops; Hiatal Hernia Repair Attempted
縮胃後胃內壓升高,加上小胃管狀構造缺乏賁門括約肌保護,出現難以控制的胃食道逆流。同年於他院進行食道裂孔疝氣修補手術,但症狀未獲改善。
Elevated intragastric pressure combined with loss of lower oesophageal sphincter protection in the sleeve led to severe, uncontrollable GERD. A hiatal hernia repair was performed at the original centre the same year — symptoms did not improve.
第 2 – 5 年 ── 長期痛苦
Years 2–5 — Prolonged Suffering
無法平躺、固體食物難以下嚥,生活品質嚴重受損
Unable to Lie Flat, Solid Food Intolerance, Severely Impaired Quality of Life
胃食道逆流持續惡化,夜間只能半坐入睡,固體食物容易卡住、嘔吐,長達數年無法正常進食或躺下休息。
Reflux continued to worsen. Nights were spent sleeping semi-upright; solid food repeatedly caused blockage and vomiting. For years she could neither eat normally nor rest lying down.
第 5 年 ── 轉介高雄長庚
Year 5 — Referred to Kaohsiung Chang Gung
腹腔鏡修正手術:疝氣完全復位 + 轉位雙通道
Laparoscopic Revision: Full Hernia Reduction + Transit Bipartition
經完整評估後,由高雄長庚體重管理中心林育弘醫師施行腹腔鏡手術,完全復位食道裂孔疝氣並轉換為 Transit Bipartition,根本解決逆流與阻塞問題。
After thorough workup, Dr Yu-Hung Lin of Kaohsiung Chang Gung Weight Management Centre performed laparoscopic revision surgery: complete reduction of the recurrent hiatal hernia and conversion to Transit Bipartition — resolving both reflux and obstruction at their root cause.
🩺 來院時的主要症狀
Presenting Complaints
🛌
無法平躺入睡
Unable to Sleep Flat
夜間逆流嚴重,數年來只能半坐或斜靠才能入睡
Severe nocturnal reflux forced her to sleep semi-upright for years
🍽️
固體食物不耐受
Solid Food Intolerance
固體食物無法順利通過,容易阻塞、嘔吐,飲食受到嚴格限制
Solids repeatedly caused obstruction and vomiting; diet severely restricted
🔥
頑固性胃食道逆流
Refractory GERD
藥物治療效果不佳,前次疝氣修補手術後症狀仍持續存在
Unresponsive to medication; persisted despite the prior hernia repair
📉
生活品質長期低落,社交、飲食、睡眠全面受影響,輾轉尋求第三意見後轉介至本中心
Quality of life severely impaired across social, dietary and sleep domains; referred after seeking a third opinion
🔬 詳細檢查與診斷發現
Investigations & Findings
入院後進行完整評估,包含胃鏡、電腦斷層及上消化道攝影(UGI series),發現以下關鍵問題:
Comprehensive workup including upper endoscopy, CT scan, and upper GI series (UGI) revealed three critical findings:
⚠️ 食道裂孔疝氣復發:Recurrent Hiatal Hernia:
原本修補的疝氣再度復發,部分胃組織再次滑入縱隔腔,造成食道與胃交接處嚴重扭曲,食物無法順利進入胃管。
The previously repaired hernia had recurred. Gastric tissue had re-herniated into the mediastinum, severely distorting the oesophagogastric junction and preventing food from passing freely into the sleeve.
⚠️ 胃出口功能性阻塞:Functional Gastric Outlet Obstruction:
疝氣導致小胃管上端受壓,固體食物「卡在門口進不去」,是嘔吐與不耐受固體食物的根本原因。
The herniated tissue compressed the proximal sleeve, creating a functional bottleneck. Solid food was "stuck at the entrance" — the direct cause of her vomiting and intolerance.
⚠️ 胃內壓升高致逆流:Elevated Intragastric Pressure Driving Reflux:
縮胃術後賁門括約肌功能喪失,加上胃管出口阻塞,胃內容物極易逆流至食道,形成惡性循環。
Loss of lower oesophageal sphincter function after sleeve gastrectomy, combined with outlet obstruction, created a vicious cycle driving gastric contents back into the oesophagus.
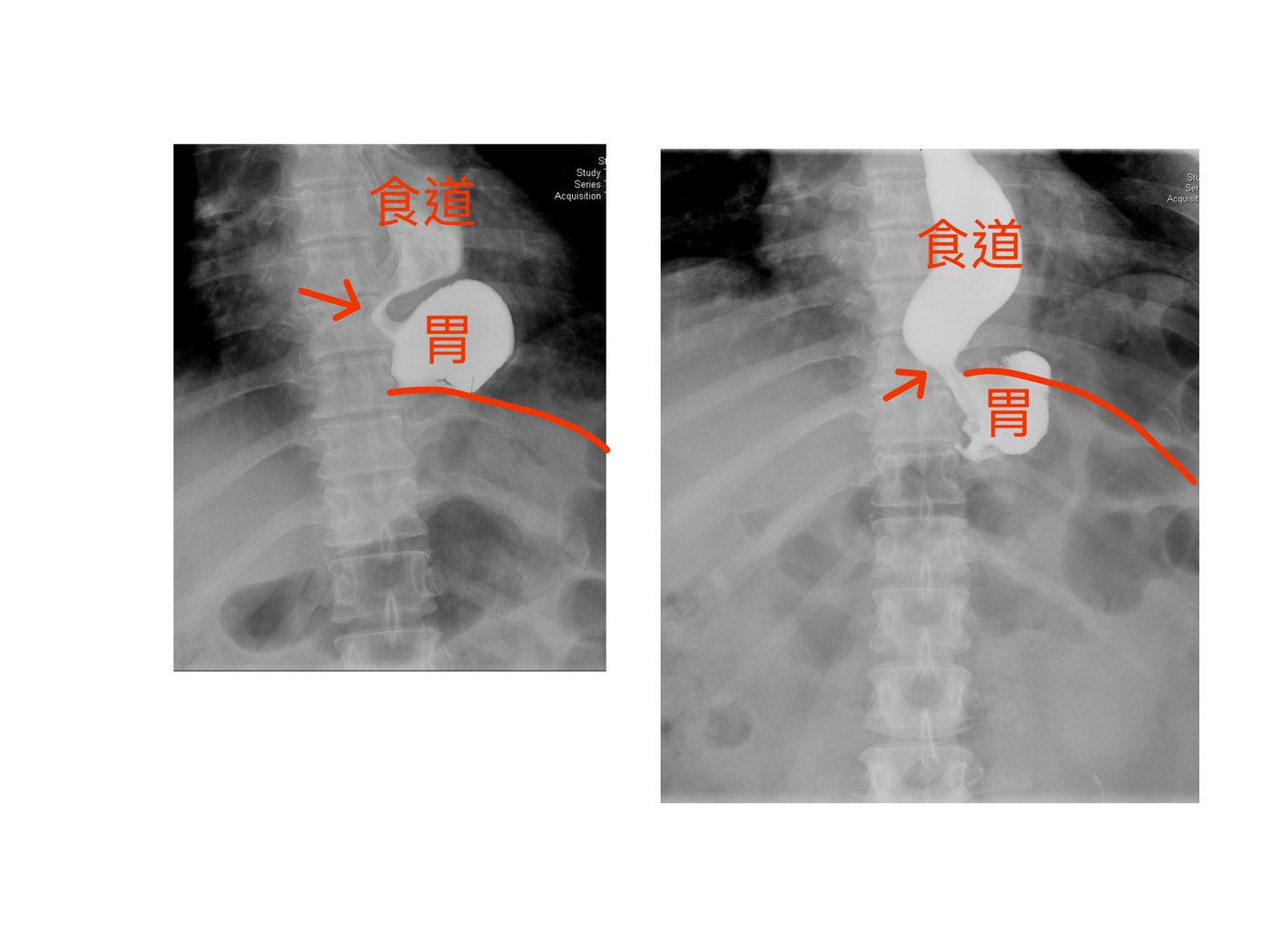
▲ 上消化道攝影(UGI):可見食道(食道)與胃(胃)的相對位置,箭頭所指為胃體滑入縱隔腔的位置,造成食道胃交接處受壓阻塞。
▲ Upper GI series (UGI): the images show the oesophagus (食道) and stomach (胃). Arrows indicate the portion of stomach herniated into the mediastinum, compressing and obstructing the oesophagogastric junction.
🔪 手術策略與執行
Surgical Strategy & Execution
本次由高雄長庚體重管理中心林育弘醫師執刀,採腹腔鏡微創手術,在術中確認疝氣範圍與胃管解剖後,依序完成以下步驟:
The procedure was performed laparoscopically by Dr Yu-Hung Lin, Kaohsiung Chang Gung Weight Management Centre. After intraoperative confirmation of hernia extent and sleeve anatomy, three sequential steps were completed:
1
完全復位食道裂孔疝氣Complete Hiatal Hernia Reduction
——將滑入縱隔腔的胃組織完整拉回腹腔,並重新修補擴大的食道裂孔,恢復正常解剖位置。
— All herniated gastric tissue was fully reduced back into the abdominal cavity and the widened hiatus was re-repaired, restoring normal anatomy.
2
解除胃出口阻塞Relief of Gastric Outlet Obstruction
——確認縮胃管狀構造暢通,移除前次手術後造成壓迫的沾黏組織。
— The sleeve lumen was confirmed patent and adhesions from the prior repair causing extrinsic compression were divided.
3
轉換術式:轉位雙通道(Transit Bipartition)Conversion to Transit Bipartition
——將原本曠置的小腸接合至縮胃管下端,形成轉位雙通道,達到胃內減壓效果,從根本上降低胃食道逆流的發生機率,同時保留正常的消化吸收功能。
— The previously bypassed jejunum was anastomosed to the distal sleeve, creating a transit bipartition. This decompresses intragastric pressure, fundamentally reducing reflux risk while preserving normal digestive absorption.
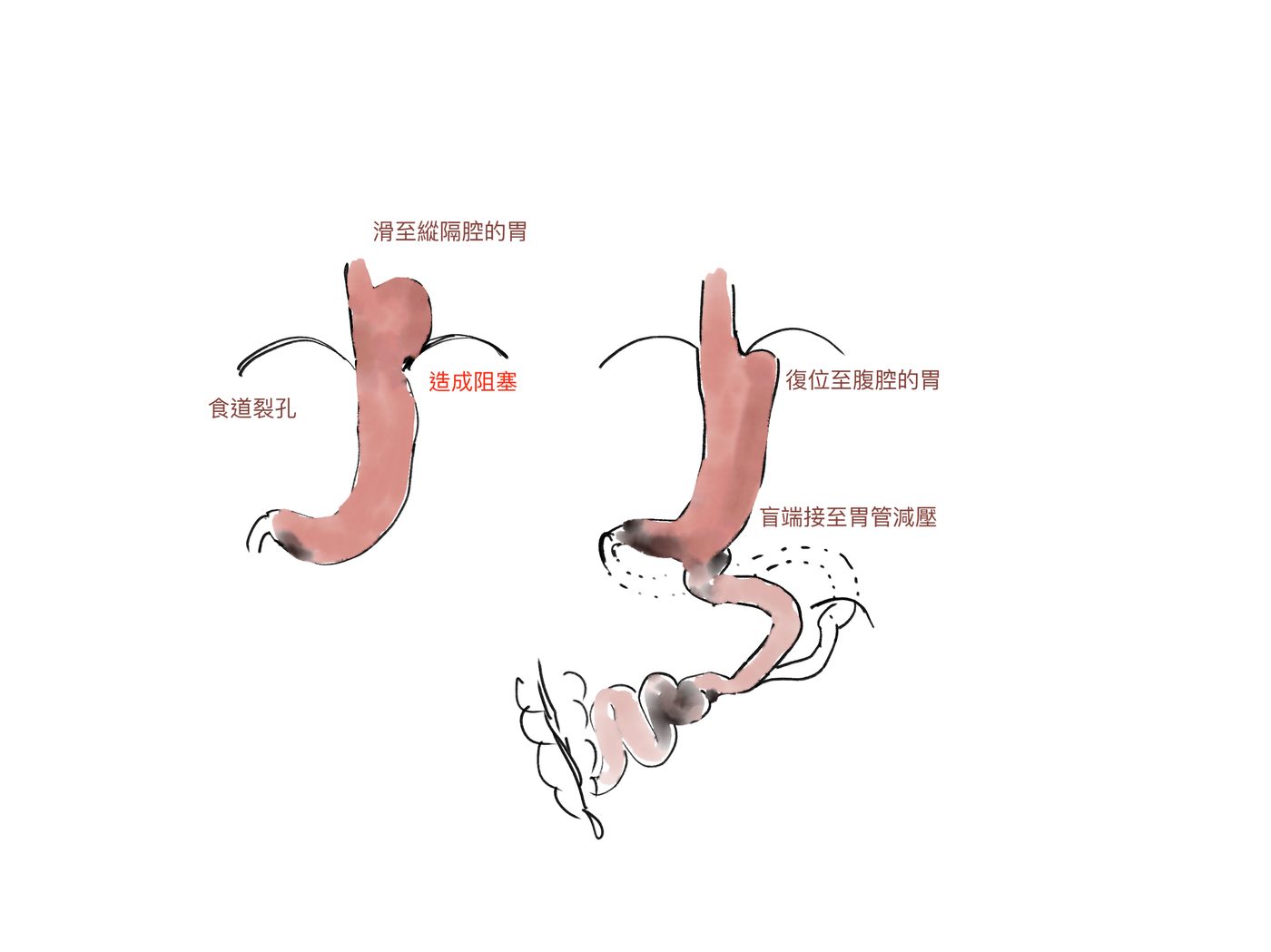
▲ 手術示意圖(左):胃滑至縱隔腔,造成食道胃交接阻塞。(右):疝氣完全復位、胃回到腹腔,盲端接至胃管下端進行減壓,完成轉位雙通道。
▲ Surgical diagram. Left: stomach herniated into the mediastinum causing oesophagogastric junction obstruction. Right: hernia fully reduced, stomach returned to the abdominal cavity, blind end connected to the distal sleeve for decompression — Transit Bipartition completed.
"
我終於能好好躺平睡一覺了!
I can finally sleep flat on my back again!
—— 術後回診時,患者的第一句話
—— The patient's first words at her post-operative follow-up
✅ 術後恢復與成果
Post-operative Recovery & Outcomes
修正手術後,患者的症狀獲得顯著改善:
Following revision surgery, her symptoms improved dramatically across all domains:
-
睡眠品質全面恢復:Sleep fully restored:
術後即可完全平躺入睡,多年來的半坐睡姿成為過去。
She could sleep flat from the first post-operative night. Years of sleeping semi-upright were over.
-
固體食物耐受正常:Normal solid food tolerance:
阻塞感消失,進食不再卡頓,飲食種類逐步恢復正常。
The sensation of obstruction resolved; diet progressively returned to normal variety and texture.
-
胃食道逆流根本改善:GERD fundamentally resolved:
轉位雙通道有效降低胃內壓,逆流頻率大幅下降,無需長期倚賴制酸劑。
Transit bipartition decompressed intragastric pressure; reflux frequency fell markedly and long-term acid suppression was no longer required.
-
整體生活品質提升:Overall quality of life restored:
可正常飲食、平躺休息,長達五年的身心消耗終於告一段落。
Normal eating, normal sleep, and relief from five years of physical and psychological exhaustion.
🏥 選擇有能力處理併發症的醫療中心Choose a Centre Equipped to Handle Complications
減重手術經過數十年演進,現今已非常安全,嚴重併發症比例極低。然而,一旦發生,通常相對棘手——疝氣復發、逆流惡化、術後阻塞,往往需要更複雜的修正手術才能解決,並非所有院所都具備處理能力。
Decades of refinement have made modern bariatric surgery very safe, with serious complication rates extremely low. However, when complications do occur, they are often complex — recurrent hernias, worsening reflux, post-operative obstruction — and require revisional procedures that not every centre is equipped to perform.
高雄長庚體重管理中心每年接受來自各地的修正手術轉診案例,擁有完整的術前評估流程與多術式修正手術經驗,是您長期安心的後盾。選擇可以終身保固的院所,才是最重要的評估標準。
Kaohsiung Chang Gung Weight Management Centre receives revisional referrals from across Taiwan each year, with comprehensive pre-operative protocols and experience in multiple revision techniques. Choosing a centre that can support you for life is the most important criterion of all.
有類似困擾?讓我們評估您的狀況
Experiencing Similar Problems? Let Us Assess Your Case.
若您曾接受減重手術但出現逆流、阻塞或其他長期困擾,歡迎前來高雄長庚體重管理中心進行完整評估。
If you have had bariatric surgery and are experiencing reflux, obstruction, or other long-term issues, we welcome you to Kaohsiung Chang Gung Weight Management Centre for a full evaluation.
⚠️ 本頁案例為真實臨床經驗分享,已去除個人識別資訊。每位患者狀況不同,手術效果與適應症需由醫師依個別評估決定。本內容僅供衛教參考,不構成醫療建議。
⚠️ This case is shared from real clinical experience with all personal identifying information removed. Individual outcomes vary; surgical eligibility and expected results are determined by physician evaluation on a case-by-case basis. This content is for educational purposes only and does not constitute medical advice.